
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
How Non-Invasive Disc Recovery Works Without Surgery
Most disc treatments keep pressure on. This one removes it—mechanically, precisely, and without cutting anything. The table creates negative pressure inside the targeted disc, which retracts bulging or herniated material away from the nerve and pulls oxygen, water, and nutrients back into tissue that's been starved of them. That's what lets the disc heal instead of just managing symptoms indefinitely.
The mechanism is specific, controlled, and engineered around one goal: creating the optimal conditions for your body to heal itself. Unlike surgery, which removes or fuses damaged tissue, non-invasive disc recovery supports the disc's natural ability to resorb herniated material and restore function. The table uses computer-controlled tension to target the affected disc level—not the entire spine—allowing for precision that basic traction tables can't achieve.
This isn't passive stretching. It's a calculated intervention that cycles between decompression and relaxation, preventing the muscles from guarding against the pull. That cycling is what allows the disc to experience genuine negative pressure—the state required for healing nutrients to move back into the damaged tissue. Most patients feel a light stretching sensation during treatment, not pain.
The results depend on two things: the severity and type of disc damage, and whether the full care plan is followed. Some patients report relief within the first few sessions as nerve pressure decreases. Lasting improvement—the kind that keeps you off an operating table—requires the disc to heal structurally, and that takes weeks, not days. This article explains how the process works, who it's for, what it requires from you, and why it's not just another "alternative" to surgery—it's often the smarter first move.
Last Updated: April 30, 2026
- What Happens Inside the Disc During Non-Invasive Recovery
- How the Decompression Table Targets Specific Disc Levels
- Why Non-Invasive Disc Recovery Isn't Just Traction
- What Conditions Respond Best to Non-Surgical Disc Therapy
- The Role of Individualized Care Plans in Disc Recovery
- What to Expect During a Non-Invasive Disc Recovery Session
- How Long It Takes to See Real Results
- Who Should Not Pursue Non-Invasive Disc Recovery
- Frequently Asked Questions
- Conclusion
What Happens Inside the Disc During Non-Invasive Recovery

Your disc absorbs shock. It's built with a tough outer ring and a gel center that cushions the bones above and below.
When it herniates or bulges, that inner material pushes out. If it hits a nerve, you get shooting pain, numbness, tingling—the kind that follows you through your entire day.
Non-invasive disc recovery creates negative pressure inside the disc. That shift does two things. First, it pulls the herniated material back, away from the nerve. Second, it draws oxygen, water, and nutrients into the disc—the resources it needs to heal but can't get when it's compressed.
Johns Hopkins Medicine confirms the body can resorb herniated material when the right conditions exist. Decompression creates those conditions mechanically.
The Disc's Natural Healing Response
Your body already knows how to heal a herniated disc.
The immune system sees the displaced material as something out of place and starts breaking it down.
The problem? Discs don't have a direct blood supply. They rely on diffusion—nutrients moving in, waste moving out, through surrounding tissue. When the disc stays compressed, diffusion stops. Healing stalls.
Surgery removes the problem tissue entirely. Non-invasive recovery gives your body the mechanical space it needs to do what it was already trying to do—resorb the herniation and restore function without cutting anything.
What Prevents Discs From Healing on Their Own
Constant compression.
Gravity, posture, repetitive motion—they all keep pressure on the disc all day long.
Rest helps. But it's not enough. Lying down reduces some load, but it doesn't create the negative pressure required to pull nutrients back in or retract herniated material.
Physical therapy strengthens surrounding muscles, which matters for long-term stability. But if the disc itself stays compressed, the structural problem remains. The pain might ease temporarily, then return the moment you go back to normal activity.
Most back pain treatments address symptoms and leave the cause alone. The disc stays compressed. The nerve stays irritated. The pain cycles back.
That's where root-cause chiropractic care makes the difference. The focus isn't managing discomfort indefinitely—it's addressing what's driving it.
The Mayo Clinic notes herniated discs are most common in the lower back and can result from age-related wear or sudden strain. The symptoms—pain, numbness, weakness—trace directly to nerve compression, not muscle soreness or generic "back pain."
How the Decompression Table Targets Specific Disc Levels
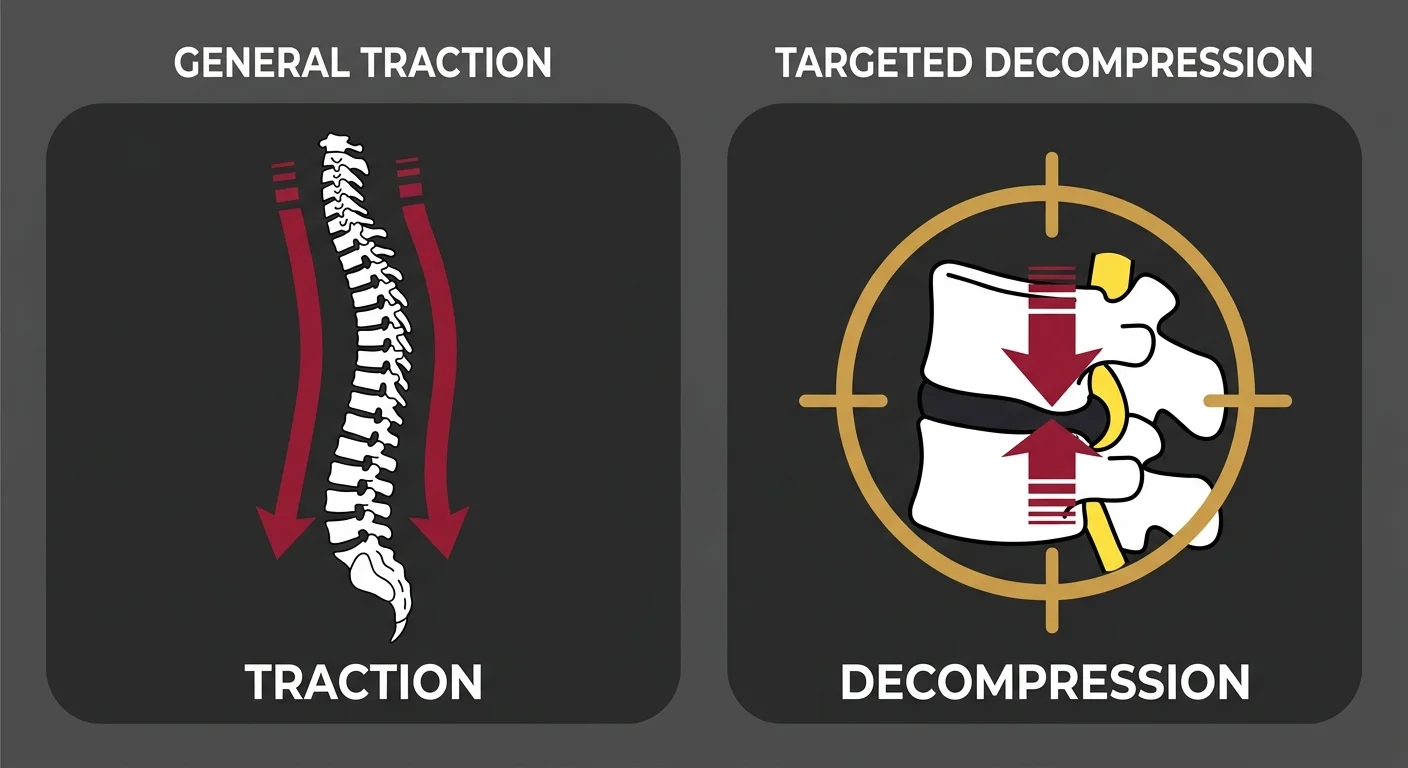
The table doesn't pull your entire spine. It isolates the disc that's causing the problem.
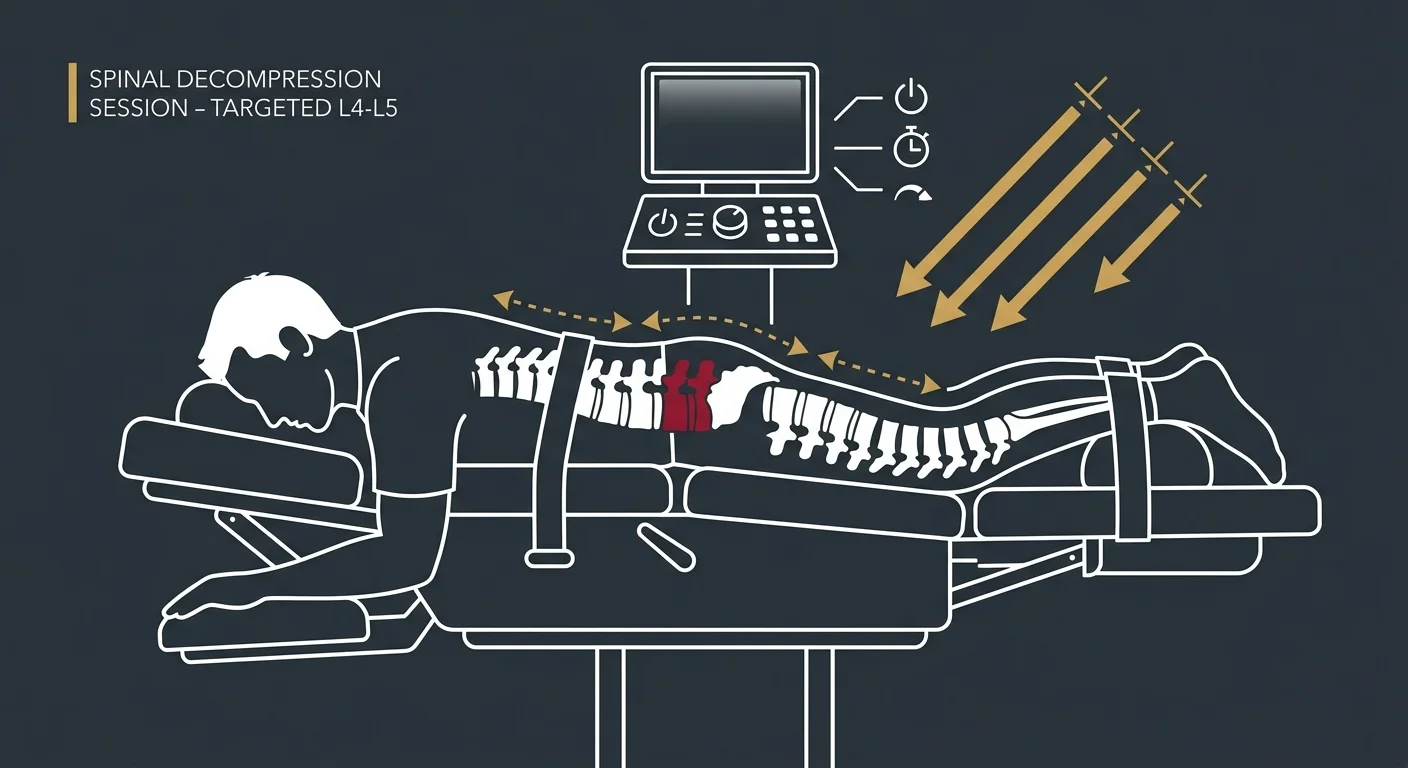
You're positioned with a harness system that anchors your pelvis or upper body depending on whether the issue's in your lower back or neck. The table applies controlled, computerized tension in cycles—pulling gently, releasing, pulling again.
That cycling prevents your muscles from fighting it. If the tension stayed constant, your body would lock up to protect itself. The on-off pattern keeps the muscles relaxed, letting the disc experience true decompression.
The computer controls the force, the duration of each cycle, the total session time. Those variables adjust based on your clinical picture—not a standard setting for every patient.
The Difference Between Manual and Motorized Decompression
Manual traction relies on the provider's judgment to apply and release tension.
It's not inherently ineffective. But it's inconsistent. The force varies. The timing varies. And it can't cycle with the precision a computer maintains.
Motorized decompression delivers the same controlled tension every time. The provider sets the parameters based on your assessment, and the table executes them exactly. If your body responds differently mid-session—if you start guarding, if the pull feels too aggressive—the settings adjust in real time.
Cleveland Clinic defines spinal decompression therapy as a non-surgical treatment using motorized traction to relieve back pain by creating negative pressure in the disc.
That precision matters because discs are delicate. Too much force risks injury. Too little doesn't create enough decompression to make a difference.
| Method | Targeting | Muscle Response | Clinical Precision |
|---|---|---|---|
| Basic Traction | Pulls entire spine uniformly | Often triggers muscle guarding | Provider-dependent, inconsistent force application |
| Non-Invasive Disc Decompression | Targets specific disc level | Cycling prevents guarding response | Computer-controlled, consistent tension with real-time adjustments |
| Manual Traction | Generalized pull, limited isolation | Variable—depends on technique | Relies on provider's physical control and timing |
Why Non-Invasive Disc Recovery Isn't Just Traction
Why the Cookie-Cutter Protocol Fails in Disc Recovery
Not every herniated disc patient gets the same table settings here.
The assessment drives the protocol—location of herniation, patient response, concurrent nerve involvement all factor in.
Some places put every back pain patient on the same decompression cycle regardless of whether it's a disc issue, a joint issue, or a muscle issue. That's not clinical judgment. That's equipment utilization.
I've seen patients transfer here after weeks on a decompression table somewhere else with zero improvement. When I reviewed their previous care, the settings were identical across every session. No adjustment based on response. No integration with other modalities. Just the same protocol, session after session, because that's what the schedule allowed.
Generic traction doesn't account for that. It assumes all spinal pain comes from the same mechanism and responds to the same intervention. That's guesswork.
A truly individualized care plan starts with what you're experiencing and builds the treatment around your clinical picture—not around what worked for the last ten patients.
Why Generic Protocols Produce Inconsistent Results
Without customization, some patients improve while others don't—not because the therapy doesn't work, but because it wasn't applied correctly for their condition.
A lumbar disc herniation at L4-L5 doesn't behave like one at L5-S1. The nerve root angle is different. The weight-bearing load is different. The surrounding tissue is different.
If the table settings don't account for that, the decompression might miss the target entirely. You're getting traction, but not where it matters.
That's the difference between a protocol and a care plan. Protocols are efficient. Care plans are effective.
What Conditions Respond Best to Non-Surgical Disc Therapy
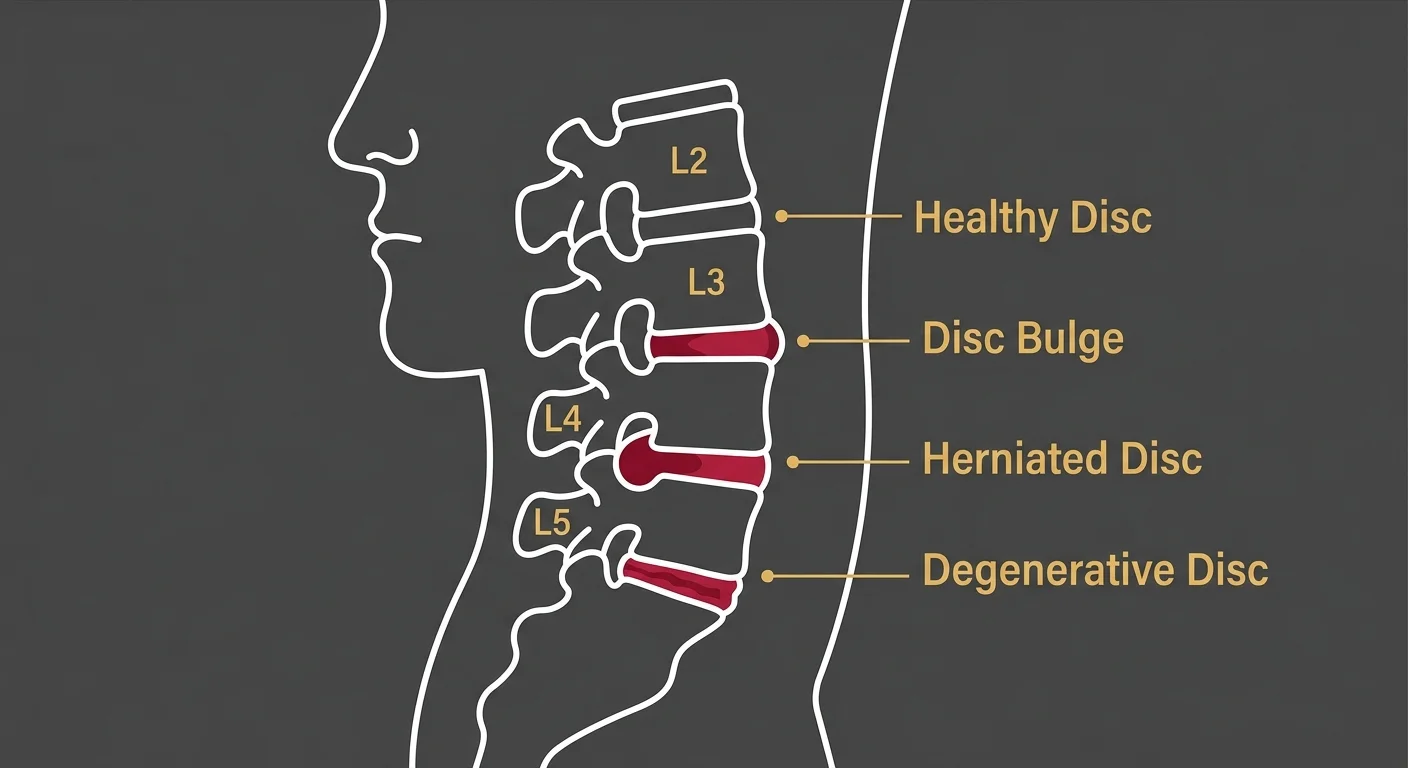
Herniated discs, bulging discs, degenerative disc disease, sciatica from disc compression—these are where decompression creates the mechanical environment for healing.
- Herniated disc — Inner gel pushes through a tear in the outer layer, presses on a nerve root, causes radiating pain, numbness, weakness.
- Bulging disc — Disc protrudes outward without rupturing, creates pressure on surrounding nerves and tissue.
- Degenerative disc disease — Disc loses hydration and height over time, leads to nerve compression and reduced spinal mobility.
- Sciatica from disc compression — Sciatic nerve is irritated by a herniated or bulging disc in the lower back, produces sharp pain down the leg.
These aren't "just back pain." They're structural problems with a nerve component. And when a nerve's involved, symptoms show up far from the actual disc injury—down your leg, into your foot, up into your shoulder or arm.
Nerve-Related Symptoms That Signal a Disc Problem
Radiating pain, numbness, tingling, weakness—these aren't muscle soreness.
They're nerve compression symptoms that often trace back to a disc pressing on a nerve root.
If you're experiencing pain that shoots down your leg when you stand or sit a certain way, that's not a tight hamstring. That's a nerve signal being interrupted by pressure at the spinal level.
If your foot feels numb or your grip strength's weaker on one side, that's a neurological symptom—not a soft tissue issue.
Nerve-related symptoms are your body's way of saying something structural is wrong. Ignoring them doesn't make them disappear. It just gives the problem more time to worsen.
Sciatica nerve pain from a disc issue is one of the most common reasons patients seek non-invasive disc recovery. The pain's severe enough to disrupt sleep, work, basic movement—but it's also one of the most responsive conditions when treated correctly.
| Disc Condition | Primary Symptoms | Why Non-Invasive Recovery Fits |
|---|---|---|
| Herniated Disc | Radiating pain, numbness, tingling in arms or legs, weakness in affected limb | Creates negative pressure to retract herniated material and relieve nerve compression |
| Bulging Disc | Localized back pain, stiffness, mild radiating discomfort, reduced range of motion | Decompression reduces outward pressure and allows disc to rehydrate and stabilize |
| Degenerative Disc Disease | Chronic low-grade pain, flare-ups with activity, stiffness after rest, gradual loss of spinal mobility | Restores nutrient flow to degenerated disc tissue, supporting long-term structural stability |
| Sciatica (Disc-Related) | Sharp shooting pain down leg, burning sensation, difficulty sitting or standing, foot drop in severe cases | Relieves pressure on sciatic nerve root by addressing disc herniation at spinal source |
Johns Hopkins Medicine explains herniated discs can heal through resorption, where the immune system breaks down and absorbs displaced disc material—but only when mechanical pressure is reduced enough to let that happen.
The Role of Individualized Care Plans in Disc Recovery
Individualized care is the standard here.
Your care plan is built from what you report and how your body responds—not from a pre-set protocol someone else designed.
Disc recovery isn't just table time. It's part of a larger clinical strategy that includes adjustments to restore joint motion, exercises to stabilize the spine, lifestyle modifications to prevent re-injury.
The decompression creates space. The rest of the plan protects it.
If the surrounding joints aren't moving correctly, the disc will stay under abnormal stress even after decompression. If the core muscles aren't strong enough to support the spine, you'll be right back where you started the first time you lift something heavy.
That's why disc recovery is never a standalone treatment. It's one component of an individualized care plan—and the plan changes if something isn't working.
Why Partial Commitment Produces Partial Results
Some patients want to pick which parts of the care plan to follow.
Show up for decompression but skip the exercises. Do the table sessions but ignore the posture corrections.
That's not partnership. That's sabotage.
If you're not willing to engage the full plan, the results won't stick. You might feel better for a few weeks, but when the structural support isn't there, the disc will re-herniate or the pain will move to a different area.
Partial commitment produces partial results. That's not a threat—it's mechanics.
If you're dealing with chronic or recurring back pain, the pattern's usually the same. Something helps for a while, then the pain comes back. That's what happens when symptoms are managed but the cause is left alone.
What to Expect During a Non-Invasive Disc Recovery Session
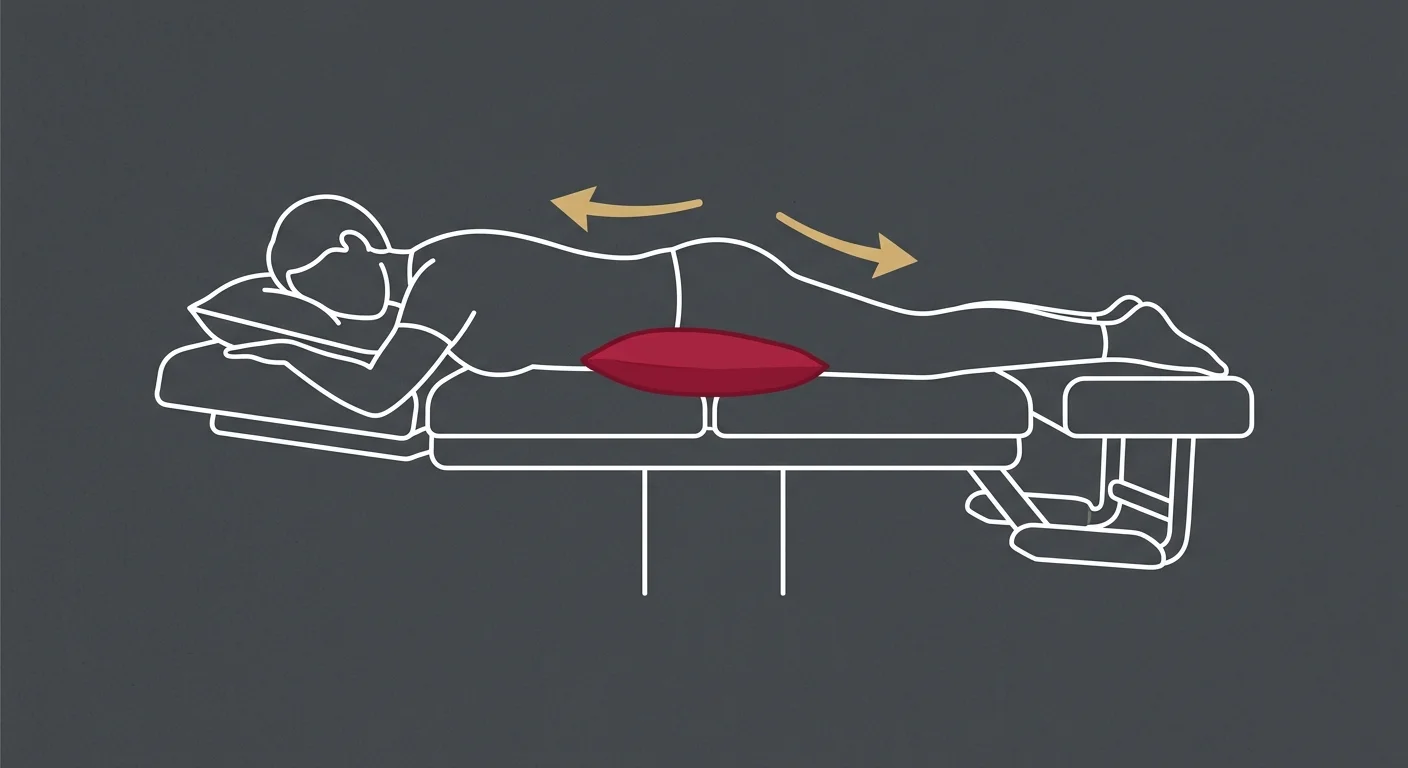
You'll be positioned on the table—face down or face up depending on whether the disc issue's in your lower back or neck.
A harness system secures your pelvis or torso to create the anchor point for decompression.
The table begins cycling through tension and release. You'll feel a gentle pulling—not painful, just noticeable. Most patients describe it as a light stretch.
Each session lasts 20 to 30 minutes. During that time, the computer adjusts the force automatically based on the pre-set protocol. If at any point the pull feels too strong or uncomfortable, the session can be paused and the settings recalibrated.
You're not sedated. You're not immobilized. You're lying on a table experiencing controlled mechanical decompression—nothing more, nothing less.
The First Session vs. Later Sessions
Initial sessions are diagnostic.
The provider watches how your body responds, adjusts tension levels accordingly, monitors for any adverse reactions.
Relief timing varies—but not randomly. If the disc's been compressed for months, you won't feel relief in one session. If it's acute, you might. The timeline matches the tissue damage, not your patience. How long the disc's been herniated and how much inflammation's present dictates when you'll notice change.
Later sessions fine-tune as healing progresses. The force might increase slightly as your tolerance improves. The cycle timing might shift. The table creates decompression. Too much risks injury. Too little does nothing. That's why the settings adjust every session—precision matters more than comfort.
| Session Phase | What Happens | What You Should Feel | Clinical Goal |
|---|---|---|---|
| Initial Assessment (Session 1-2) | Provider establishes baseline settings, monitors patient response, identifies contraindications | Light stretching sensation, possible mild soreness after first session | Determine safe decompression parameters and confirm treatment appropriateness |
| Active Treatment (Session 3-12) | Controlled cycles of tension and release, gradual increase in decompression force as tolerance builds | Gentle pulling, relief of nerve pressure symptoms, reduced radiating pain | Create sustained negative pressure to retract herniated material and restore nutrient flow |
| Stabilization (Session 12+) | Fine-tuning of settings, integration with corrective exercises and spinal adjustments | Continued symptom improvement, increased functional mobility | Support structural healing and prevent re-injury through coordinated care plan |
| Maintenance (As Needed) | Periodic decompression sessions to address flare-ups or prevent recurrence | Minimal to no discomfort, preventive benefit | Maintain disc health and spinal function long-term |
How Long It Takes to See Real Results
Many patients feel some relief within the first few sessions as nerve pressure decreases.
That's not healing—that's decompression working mechanically.
Real healing—the kind that keeps you functional long-term—takes weeks. The disc has to resorb material, re-establish nutrient flow, stabilize structurally.
A typical care plan runs 12 to 20 sessions over 4 to 6 weeks, but that's a baseline. Some conditions require more time. Some require less. The timeline's built from your assessment, not a calendar.
If you've tried injections or PT and the pain came back, that's because those approaches managed symptoms without addressing the disc pressure itself. Decompression creates the structural environment for healing. The difference is mechanical, not theoretical.
The National Institutes of Health published a comparison of surgical and non-surgical treatment outcomes for lumbar disc herniation. The data showed that while surgery produced faster initial relief, non-surgical approaches—including spinal decompression—achieved similar long-term functional outcomes without the risks and recovery time of an invasive procedure.
What Happens After the Initial Care Plan
Once the disc's healed to the point where nerve pressure is resolved and function is restored, the focus shifts to maintenance.
That doesn't mean weekly decompression sessions for the rest of your life. It means exercises to keep the core strong, posture corrections to reduce abnormal loading, periodic check-ins to catch early signs of re-injury before they escalate.
Some patients return for occasional decompression sessions if they experience a flare-up after heavy lifting or prolonged sitting. That's not a failure—it's preventive care.
The goal is to get you to a point where you don't need the table anymore. Honest, outcome-based care plans are built around discharge, not indefinite retention.
Who Should Not Pursue Non-Invasive Disc Recovery

Severe osteoporosis, spinal fractures, tumors, advanced spinal instability—these are conditions where decompression isn't safe or appropriate.
- Severe osteoporosis — Bone density's too low to withstand even gentle traction forces.
- Spinal fracture — Any existing fracture must heal completely before decompression can be considered.
- Spinal tumor — Pathological changes in the vertebrae or surrounding tissue make decompression contraindicated.
- Advanced spinal instability — Conditions like spondylolisthesis with significant slippage require surgical stabilization, not mechanical decompression.
- Pregnancy (case-dependent) — While not an absolute contraindication, decompression during pregnancy requires additional clinical evaluation.
- Aneurysm or severe vascular disease — Increased pressure changes during decompression could pose cardiovascular risk.
These aren't gray areas. If you have one of these conditions, decompression isn't an option. The assessment process is designed to identify these contraindications before they become complications.
Why Assessment Always Comes First
No one gets on the table without a full clinical evaluation.
That's not a formality. That's how contraindications are identified before they become complications.
The assessment includes detailed history, orthopedic and neurological testing, often imaging to confirm the disc diagnosis and rule out other pathology.
If decompression isn't appropriate for your condition, that's information you deserve to have up front—not after you've committed to a care plan that won't work.
If you're considering spinal fusion surgery and want to know if non-invasive recovery is a viable alternative, the assessment will answer that.
If you're wondering whether healing a herniated disc on its own with specialized care is possible, the clinical findings will tell you if your case fits that profile.
Spine-health provides a comprehensive overview of nonsurgical treatments for herniated discs, including physical therapy, medications, injections, spinal decompression—each with specific indications and contraindications that must be evaluated case-by-case.
Frequently Asked Questions
How is non-invasive disc recovery different from simple spinal traction?
Unlike basic traction which pulls the entire spine, non-invasive disc recovery uses computer-controlled tension to target a specific disc level, allowing for a more precise and gentle decompressive effect.
Basic traction applies a generalized pull across the spine without isolating the problem area. That makes it less effective for disc-specific conditions and more likely to trigger muscle guarding.
Non-invasive decompression cycles the tension on and off, preventing your muscles from resisting the pull. That's what allows true negative pressure to develop inside the disc—something constant traction can't achieve.
The computer controls the force, the timing, the total session duration. Those variables adjust based on your clinical picture, not a standard protocol applied to every patient.
How long does it take to see results from non-invasive disc therapy?
While many patients report some relief within the first few sessions, a full care plan is typically necessary to achieve lasting functional improvement as the disc heals over several weeks.
Early relief is usually nerve pressure decreasing as the disc retracts away from the nerve root. That's a mechanical response—not structural healing.
Structural healing—the kind that prevents the pain from returning—takes time. The disc has to resorb the herniated material, restore nutrient flow, stabilize under normal loading conditions. That process happens over weeks, not days.
A typical care plan runs 12 to 20 sessions over 4 to 6 weeks, but the timeline's built from your assessment and response to treatment—not a fixed schedule.
Is non-surgical disc recovery painful?
No, the process is designed to be gentle and comfortable. Most patients feel a light stretching sensation in their back or neck during the session.
You're positioned on the table with a harness system that creates the anchor point for decompression. The table applies controlled tension in cycles—pulling gently, releasing, pulling again.
That cycling prevents muscle guarding and keeps the decompression comfortable. If at any point the pull feels too strong, the session can be paused and the settings adjusted.
Some patients experience mild soreness after the first session—similar to what you'd feel after a new exercise routine. That's normal and typically resolves within 24 hours.
Can a disc heal permanently without surgery?
Yes, with the right conditions, the body can resorb herniated disc material. Non-invasive therapy creates an ideal environment to facilitate this natural healing process. If you want to understand the specific mechanisms behind healing a herniated disc on its own, that question's addressed in detail elsewhere.
Johns Hopkins Medicine explains the immune system recognizes displaced disc material as foreign tissue and begins breaking it down through resorption. But that only works if mechanical pressure is reduced enough to let it happen.
Decompression creates negative pressure inside the disc, which retracts the herniated material and draws in oxygen, water, nutrients. That's the environment the body needs to complete the healing process on its own.
Surgery removes the problem tissue entirely. Non-invasive recovery supports your body's ability to do what it was already trying to do—heal the disc naturally without cutting anything.
The results are permanent as long as the underlying cause—abnormal loading, poor posture, weak core stability—is addressed through the full care plan.
Who is not a good candidate for non-invasive disc recovery?
Patients with conditions like severe osteoporosis, spinal fractures, tumors, or certain advanced spinal instabilities may not be suitable candidates, which is determined during a thorough assessment.
Severe osteoporosis means the bones are too fragile to withstand even gentle traction. Spinal fractures must heal completely before any decompression can be considered. Tumors or other pathological changes in the spine make decompression contraindicated.
Advanced spinal instability—like spondylolisthesis with significant slippage—requires surgical stabilization, not mechanical decompression.
These aren't gray areas. If you have one of these conditions, the assessment will identify it before you're placed on the table.
The evaluation includes detailed history, orthopedic and neurological testing, often imaging to confirm the disc diagnosis and rule out other pathology. If decompression isn't appropriate for your condition, that's information you deserve to have up front.
Conclusion
Surgery removes or fuses. Non-invasive disc recovery supports your body's ability to heal itself.
That's not a lesser option. For the right candidate, it's the logical first move—one that avoids the risks, recovery time, permanent structural changes that come with spinal fusion.
The process works when the clinical picture supports it and when the patient commits to the full plan. Half-measures produce half-results.
If you've been told surgery's your only option and you're in Morton or the surrounding area, it's worth finding out if your disc can heal without it.
Real answers are more valuable than comfortable ones. If decompression isn't appropriate for your condition, that's information you deserve to have before you commit.
But if it is—and you've been living with nerve pain, radiating symptoms, restrictions that are keeping you from your life—this is a conversation worth having.
If your disc pain's followed you through every standard recommendation and surgery feels like the only option left, that's worth a real conversation.
An assessment at Touch of Wellness Chiropractic starts with what you're experiencing—not a protocol someone else designed. The evaluation will tell you if non-invasive disc recovery's appropriate for your condition, what a realistic care plan looks like, what you'll need to do to protect your spine after treatment.
If you're considering spinal fusion surgery and want to know if non-invasive recovery's a viable option, the assessment will give you a clear answer. If you're in Morton, Peoria, or the surrounding area, see what your assessment looks like.
Unexplained doesn't mean it's not real. And dismissed doesn't mean it's not treatable. It just means no one's looked at the right thing yet.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet